Program Evaluation
Parent training programs rarely have an explicit focus on improving parenting practices, parent problem-solving, or stress management (Brookman-Frazee et al, 2006). Along with increased self-efficacy, these are all aspects of parent empowerment. A focus on parent empowerment and psychological acceptance are particularly appropriate for many low and middle income countries, where mothers often shoulder full responsibility for both care and education of their children with disabilities in addition to the demands of the family and household. In addition, there is often a deeply entrenched belief that parents should not question teachers and other professionals. Teaching parent skills and increasing parent knowledge alone is not sufficient to shift these powerful dynamics. The Parent Child Training Program (PCTP) was developed in India in 2000 with parental acceptance of the child and empowerment as explicit program goals. The program additionally aims to provide practical and theoretical knowledge on autism and behavior management. Training takes place over a 9to 12 week period, with the parent and child attending together. To date, the PCTP has trained over 500 participants.
Following guidelines for evaluation of parent training programs (Matthews and Hudson, 2001), the RAFIN PCTPevaluation was developed to 1) examine whether the program design and implementation have a sound theoretical basis; 2) the extent to which the program objectives have been met; and 3) to determine the extent to which the parenting skills acquired through the training have transferred to other situations and maintained over time.
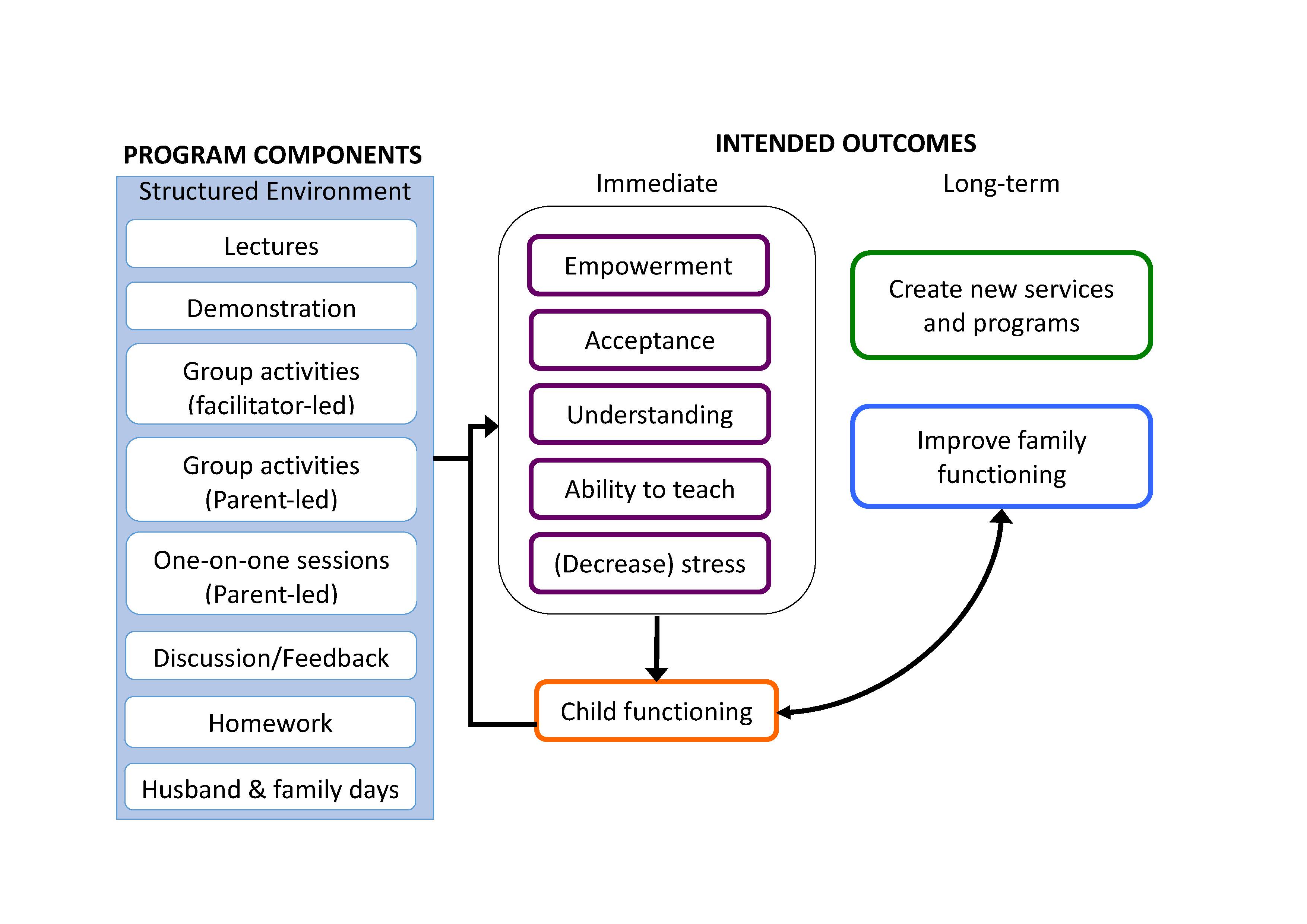
The underlying model of the PCTP is as follows:
Three consecutive cohorts of families (n=48 total) are participating in the evaluation. Participants joined from a wait-list and entered on a first-come, first-served basis. Diagnosis was confirmed using the ADOS and SCQ. Both parents were interviewed at the start and end of the program. Mothers were again interviewed eight months after their completion of the program, and follow up at 15 months after the intervention is ongoing. Measures consist of a combination of 1) standardized, Western instruments 2) tools developed specifically for this evaluation, and 3) qualitative data collection through coding of videotape and audiotape data.
Cohorts were not different in demographic characteristics or outcome measures at baseline. Results from the comparisons between the pre- and post-intervention showed significant increases across measures. The statistically significant gains achieved by the post-test were maintained across all parent outcome measures at eight months, including empowerment, acceptance, knowledge of autism, sense of competence, and decreased stress (all p<.001). In addition, parent empowerment significantly increased between the post-test and follow up period (p<.01). Mothers were able to articulate gains they perceived in their children and in their own lives in response to open-ended questions at eight months.
The PCTP was developed specifically to meet the needs of families in India, where disability remains highly stigmatizing and services are limited. Using both standardized measures and those developed for this study, the current evaluation provides an estimate of project impacts in key parent outcomes eight and fifteen months following the completion of a training program. The acceptance and empowerment focus of this model offers a novel way to conceptualize parent training, adds value to knowledge and behavioral training alone, and has high relevance for families in situations where cultural, economic and other contextual factors may be similar to those in India.


